

")
Post by Danica Helms, a post-baccalaureate student with a degree in Biology. Danica is completing a Bachelor’s of Science in Psychology with a minor in Interdisciplinary Neuroscience at Portland State University. She is passionate about women’s health, the psychological implications of societal pressures, and how gendered stereotypes negatively impact women’s reproductive, emotional, and mental well-being.

Note to reader: While acknowledging gender diversity and genetic variations, due to the simplicity of this post, I will primarily reference the sex of individuals. With regards to women, that includes females (AFAB, or “assigned female at birth”), and individuals with female reproductive organs.
Outreach!
My strongest ability has always been expressing my knowledge through my love of writing; however, I’ve always struggled to verbally express my ideas. This outreach through Northwest Noggin was a remarkable experience that allowed me to demonstrate my understanding and passion while gaining key skills in public speaking.

One of my favorite aspects of outreach was learning about each volunteer’s unique experiences and expertise, which brought a diverse set of skills and knowledge. I was also humbled by the types of questions students, even elementary students, asked.

During our many school visits, I spoke, inquired and collaborated more and more, and actually retained what I learned better than I did in a traditional classroom setting.
I Wanna Touch a Uterus!
During outreach to Columbia City Elementary, we excitedly announced that kids could come look at human and animal brains. A young boy exclaimed, “I wanna touch a uterus!”
Kids of all ages are curious about bodies; this is why comprehensive reproductive health education is important for everyone. No matter what, everyone will know an individual who has female reproductive organs, whether it’s their mom, sister, friend, girlfriend/wife, daughter, or just someone you work with. Women’s health is frequently under-mentioned, significantly understudied, and certain aspects are considered taboo, which creates shame, guilt, and stigma affecting women.

Comprehensive Reproductive Health Education
I cannot provide full coverage of reproductive health education in a short post. Nevertheless this topic should be emphasized due to its crucial importance for the emotional and mental well-being of women.
Growing up, I had the worst menstrual symptoms: heavy cycles, severe cramps, difficulty regulating emotions and embarrassment. I also believed that a woman could get pregnant at any time throughout the month. I was continuously stressed and anxious about an unwanted pregnancy.
Comprehensive reproductive health education provides emotional support, increasing confidence, knowledge, autonomy, norms about sex and access to resources. Greater menstrual health knowledge is linked to lower menstruation-related stress and higher self-efficacy. Education can also play a crucial role in lower-income communities, where knowledge can help reduce stress tied to socioeconomic differences.
Research finds that lower menstrual health knowledge, a lack of supplies or privacy, severe menstrual pain, and lower self-efficacy are associated with significantly worse mental health outcomes. Existing education is often limited, and primarily focused on hygiene and menstrual cycle changes (excluding ovulation), and not how the menstrual cycle is connected to women’s health and well-being.
Early reproductive education has meaningful emotional and developmental benefits when it’s open, supportive, practical, and includes accessible resources.
LEARN MORE (Recommended): It’s Your Body: The Young Women’s Guide to Empowered Sexual Health
LEARN MORE: Everyone needs to be educated’: pupils’ voices on menstrual education
Hormones and Neurotransmitters Shape the Brain
Sex differences within the brain are less pronounced at birth, but increase during puberty, shifting again in adulthood, and again later in life. Differences in genes and gene expression and variation in hormones, enzymes, receptors (including receptor sensitivity, density and distribution) contribute to extensive potential diversity.

Estrogen is the dominant hormone for female development, characteristics, and regulation of menstrual cycles. Estrogen promotes synaptogenesis (increases in nerve connectivity) and memory. Reductions in estrogen across the menstrual cycle can cause cognitive symptoms including mood changes, fatigue, brain fog, decreased working memory, higher stress, and impaired emotional regulation.
Progesterone is a hormone released after ovulation, and is responsible for preparing the uterus by thickening its lining for the implantation of a fertilized egg (pregnancy). During menstruation, decreased levels of progesterone impact the brain by causing hyper-responsivity to stress, creating anxiety and irritability. Women can experience lapses in concentration, increased emotional sensitivity, greater amygdala reactivity, and more difficulty maintaining deep sleep.
Serotonin and dopamine are both neurotransmitters, crucial chemical messengers in the brain. Serotonin regulates mood, sleep cycles, and gut health, promoting feelings of satiation and well-being. Dopamine assists in motivation, anticipation, and is part of our brain’s reward system, improving cognitive alertness, mood, and learning.
Higher levels of these two neurotransmitters (beginning in the follicular phase) are linked to higher energy and improved mood, increased motivation, increased libido, along with better cognitive and memory function. Lower levels of these neurotransmitters in the luteal phase are linked to a drop in mood, creating symptoms of depression and anxiety, irritability, reduced motivation, and brain fog.
LEARN MORE: Sex hormones affect neurotransmitters and shape the adult female brain during hormonal transition periods
LEARN MORE: Estrogen Effects on Cognitive and Synaptic Health Over the Lifecourse
LEARN MORE: Estrous cycle and stress: influence of progesterone on the female brain
LEARN MORE: Physiology, Progesterone
LEARN MORE: Progesterone- Cleveland Clinic
LEARN MORE: Serotonin and Dopamine: Unifying Affective, Activational, and Decision Functions
Bodies are amazing!
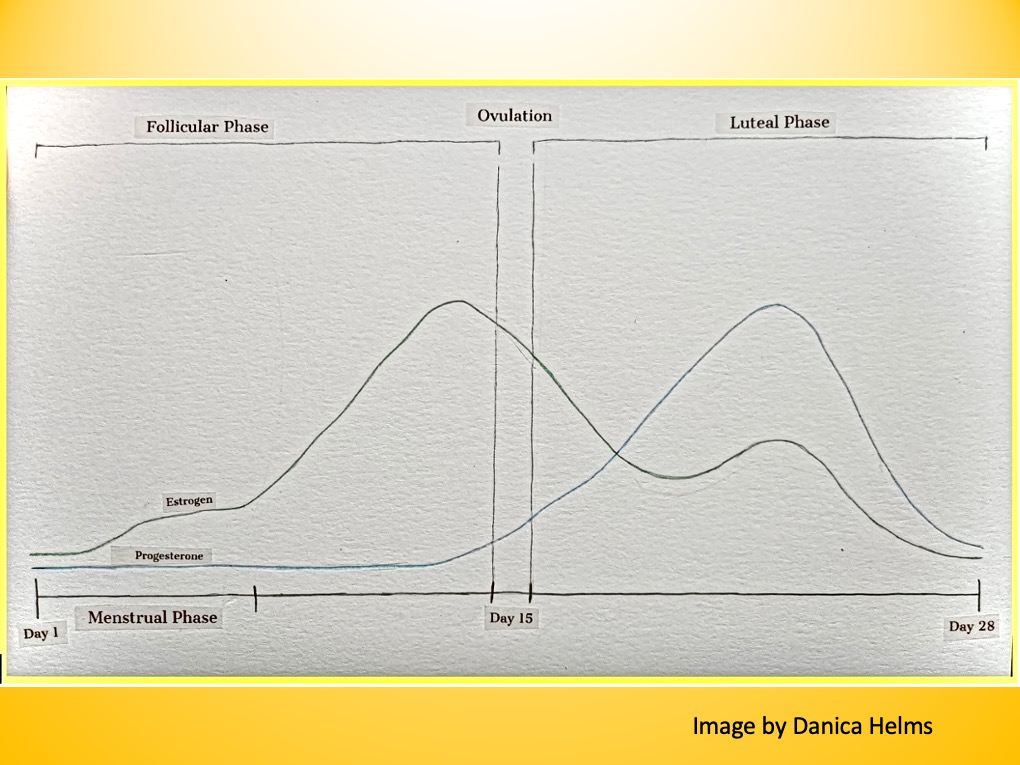
The menstrual cycle is a natural hormonal and physical process for individuals with female reproductive organs, where the body prepares the uterus and ovaries for a potential pregnancy.
The average menstrual cycle in women lasts approximately 28 days, resulting in either menstruation, where our bodies shed their prepared uterine lining, or a pregnancy.
However, menstrual cycles are rarely the stereotypical “ideal” 28 days. They vary between 23-35 days depending on the individual, their age, and a host of lifestyle variations. If you’re a woman remember that it’s your body, and variations in individuals with female reproductive organs most certainly exist when determining the length of each portion of the cycle.
LEARN MORE (Recommended): It’s Your Body: The Young Women’s Guide to Empowered Sexual Health
Menstrual Phase
Days 1-6 of your cycle, duration is variable.
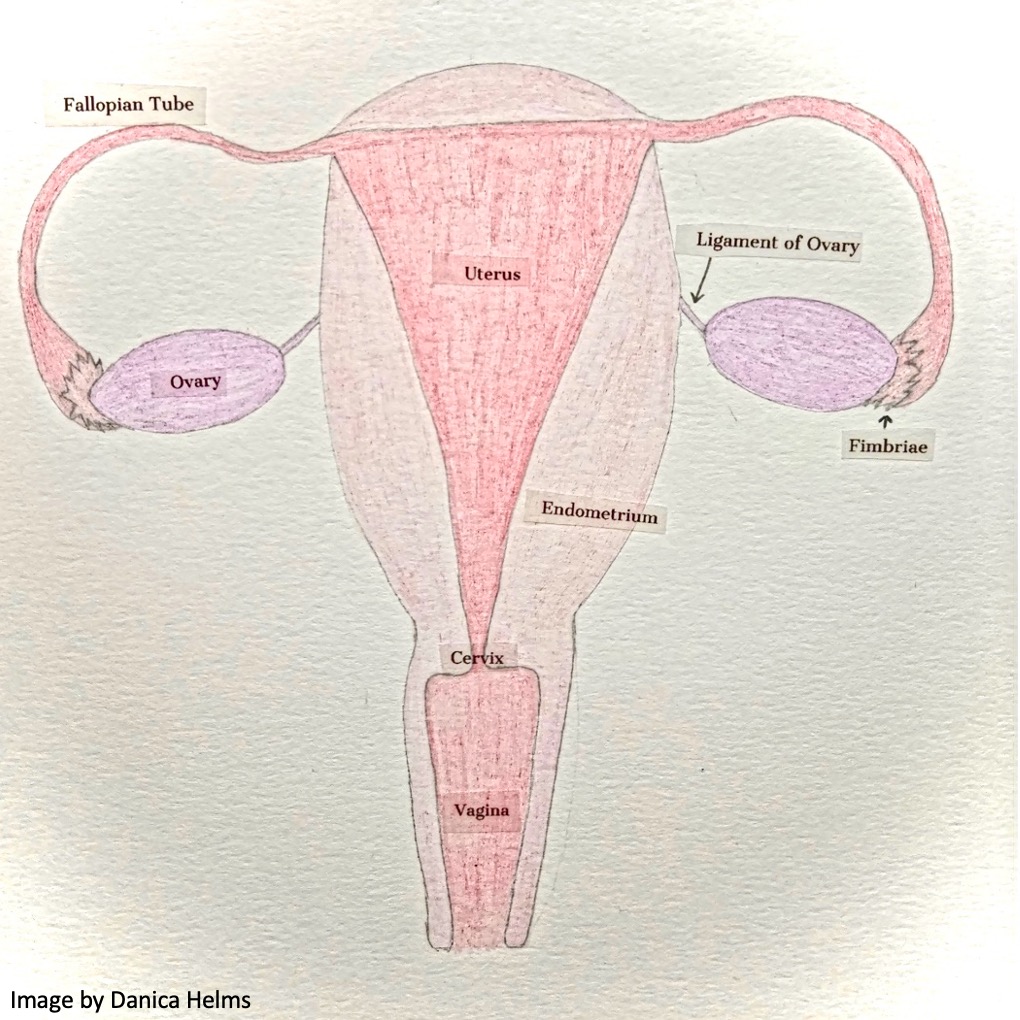
This is when there is a rapid decline in estrogen and progesterone levels, causing your uterus to shed its lining, and bleeding to begin. The actual uterine lining, known as the endometrium and the endometrial glands, is shed during this phase. The uterine muscle, known as myometrium, is responsible for the contractions that facilitate period cramps and the removal of the lining.
Fun Fact: Our cervix drops to a lower position in the vaginal orifice and ever so slightly dilates during this time to release the blood out of the uterus.
LEARN MORE: Physiology, Menstrual Cycle
LEARN MORE: Novel microarchitecture of human endometrial glands
Follicular Phase (Proliferative Phase)
Days 7-12 of your cycle, duration is variable.
The follicular phase begins on day one of your period, however, hormone levels gradually rise at the end of each individual’s menstruation period to support maturing follicles, ending with ovulation.
During this time, your body undertakes its “monthly subscription” of preparing for conception. The follicule-stimulating hormone (FSH) promotes the maturation of ovarian follicles (eggs) by producing estrogen and stimulating the production of progesterone. As expected, your body begins creating a fresh, thick uterine lining for the preparation and expectation of pregnancy.
Fun Fact: Mature female egg cells are considered the largest cell in the human body.
LEARN MORE: Proliferative and Follicular Phases of the Menstrual Cycle
Ovulatory Phase (highly fertile)
Days 13-19 of your cycle, duration is variable.
This phase formally begins 1-2 days before ovulation, when your body spikes in luteinizing hormone (LH) and your estrogen and testosterone are also at their peak, causing your ovary to release a mature egg into the fallopian tube around day 15.
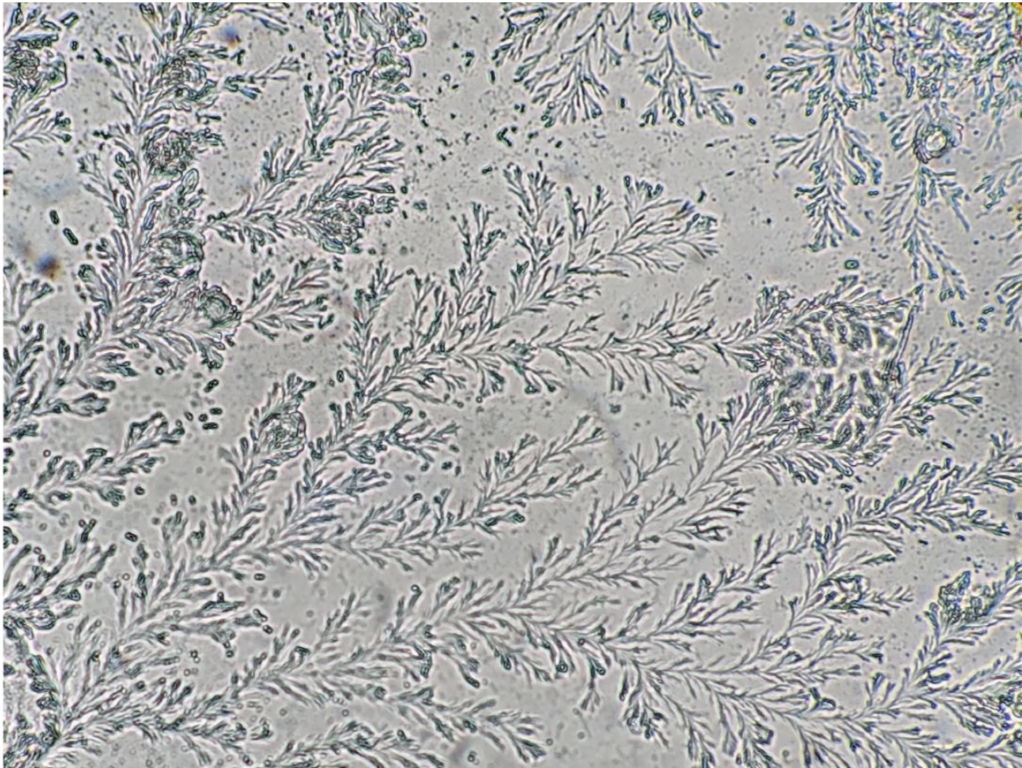
IMAGE SOURCE: Your Cervical Mucus Is Beautiful
Fun Fact: Contrary to popular belief, you are only fertile for about one week a month. Due to the high peak in estrogen, your body produces a stretchy discharge resembling egg whites. Under a microscope, this discharge has a fern-leaf pattern, acting as a way to help sperm travel into the cervix and reach the fallopian tubes, where conception occurs. Even under a microscope the female body is remarkable.
LEARN MORE: Physiology, Ovulation
Luteal Phase (Secretory Phase)
Days 15-28, or until menstruation begins, this phase duration is quite variable.
This phase begins directly after ovulation to prepare the uterus for implantation of a fertilized egg. If conception does not occur, estrogen and progesterone levels decline in preparation for menstruation. This is when premenstrual syndrome (PMS) symptoms occur.
Fun Fact: Due to high levels of progesterone in the preparation for implantation, this phase’s discharge becomes thick and sticky (white/creamy) which acts as a barrier against bacteria to protect the uterus; if no pregnancy, hormones decline rapidly where menstruation occurs.
LEARN MORE: What is the luteal phase of the menstrual cycle?
LEARN MORE: Luteal Phase Discharge: What It’s Telling You
LEARN MORE: What is premenstrual syndrome (PMS)?
The impact of menopause
Later in life, estrogen levels significantly drop (and also fluctuate) during perimenopause, and then crash during menopause, creating a spectrum of biological changes that can affect women’s overall health.
Once again, low estrogen can cause cognitive symptoms. During this time, women might experience mood changes, hot flashes and/or night sweats, muscle discomfort, and difficulty concentrating. Women are also at an increased risk of bone loss, cardiovascular complications, and are more likely to develop Alzheimer’s disease when their estrogen levels decline, if not properly monitored.
“Postmenopausal women experience a steeper decline in TCV (total cortical volume) and GMV (grey matter volume) compared to pre/perimenopausal individuals, implying that sex hormones may have a direct effect on brain growth patterns” – Brain volumetric changes in menopausal women
LEARN MORE: What Is Menopause?
LEARN MORE: Management of the Perimenopause
LEARN MORE: Sex differences in brain structures throughout the lifetime
LEARN MORE: Integrative structural, functional, and transcriptomic analyses of sex-biased brain organization in humans
LEARN MORE: Menopause and women’s cardiovascular health: is it really an obvious relationship?
Disparities, Socialization, and Gender Expectations
Biology alone never explains outcomes.
Women are underrepresented in healthcare and research, leading to male-centered treatment data, diagnostic criteria, and drug dosing that don’t always reflect women’s physiology. Providers frequently take women’s symptoms, especially pain, less seriously, which negatively influences treatment urgency and outcomes. Additional barriers such as race, income, education, and insurance status play a crucial role in medical access, quality, and health outcomes that often worsen disparities between women and men, adding to existing inequalities in diagnosis and care.
In 2025 the Trump administration actually BANNED the terms “woman” and “women” from NIH research grant applications!
LEARN MORE: Growing number of federal health agencies are combing grants for taboo words
LEARN MORE: What happens to health research when ‘women’ and ‘diversity’ are banned words?
LEARN MORE: ASU researcher on the importance of considering sex differences in health studies
LEARN MORE: Can you get a yeast infection from antibiotics?
I find it particularly unacceptable that a “research” article, now thankfully retracted, secured funding for a study titled “Attractiveness of women with rectovaginal endometriosis: a case-control study.”
“I fail to understand how a small group of Italian doctors rating attractiveness of women with different stages of endometriosis contributes anything to medical science.” –Dr. Jennifer Gunter
Endometriosis causes severe, debilitating pain, and yet these “researchers” studied attractiveness as if women were objects. It is dehumanizing when the subject of study is framed around attractiveness when attached to a debilitating condition. These studies focus their attention away from pain, suffering, and unmet clinical needs and instead reinforce sexist behaviors.
Under-prioritizing women’s pain and serious outcomes is failing women’s health.
LEARN MORE: ‘Disgusting’ study rating attractiveness of women with endometriosis retracted by medical journal
LEARN MORE: Endometriosis: A Review of Clinical Diagnosis, Treatment, and Pathogenesis
Another example of a failure to properly include women concerns ADHD and Autism, which were often seen as “boy disorders” and based on stereotypical male behaviors. This created barriers, with women often experiencing diagnostic delays or misdiagnoses due to symptoms varying from male norms.

Women often camouflage or mask during social interactions, internalizing their emotional difficulties. When coupled with unavailable and/or unaffordable diagnostic services, this can prevent early diagnosis. Those with behavioral difficulties may increase their chance to get medical attention; however, many are first diagnosed with attention-deficit disorder (ADD) or ADHD, bipolar disorder, depression, anxiety, or obsessive-compulsive disorder (OCD) before receiving an evaluation for autism.
LEARN MORE: Does camouflaging predict age at autism diagnosis? A comparison of autistic men and women
Health policies also frequently fail to reflect women’s specific health needs.
Women have a higher prevalence of conditions such as chronic pain and autoimmune diseases, and are more likely to develop depression or PTSD than their male counterparts. Stress, socioeconomic inequalities, and societal pressures all contribute to women’s health disparities by increasing cortisol and inflammation. Over time, this can lead to a higher risk of heart disease, a weakened immune system, hormonal disruptions, sleep problems, and chronic pain conditions.
Women are all disproportionately exposed to caregiving burdens and gender discrimination which are linked to worse long-term health outcomes. Biological sensitivities to chronic stress can affect women by disrupting their menstrual cycle and fertility.
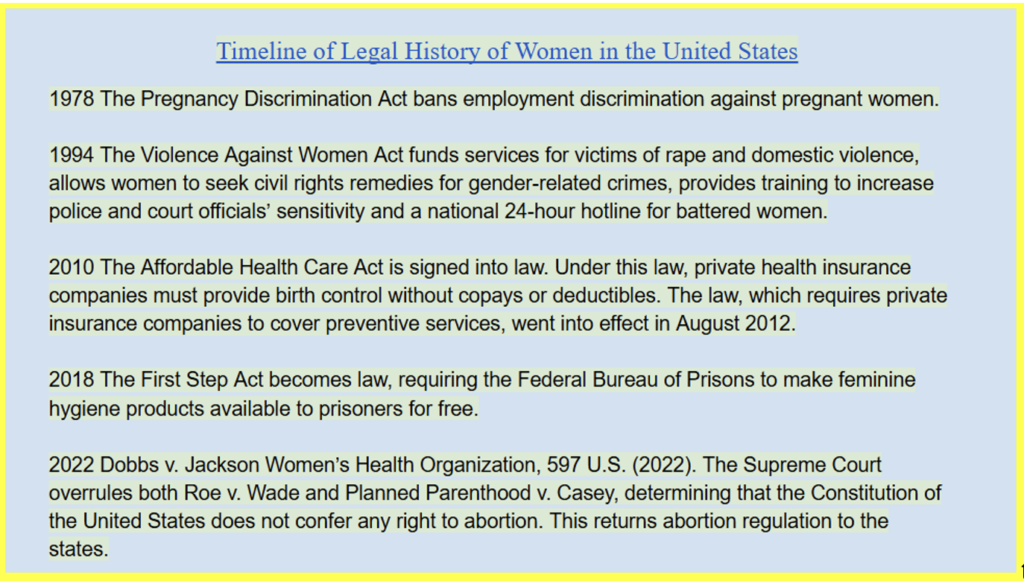
LEARN MORE: Timeline of Legal History of Women in the United States
In addition, reproductive societal pressures historically place women as the only reason fertility issues occur. However, male fertility also plays a role. Current research help shifts the stigma away from women by revealing that sperm quality and reproductive function decline as men age, resulting in increased risk of sperm DNA damage, miscarriage, and some genetic conditions. Reproductive outcomes are influenced by both partners’ biology, not just the mother’s.
LEARN MORE: Fertility and the Aging Male
LEARN MORE: Yes, men have a biological clock too. But it’s not just age that affects male fertility
LEARN MORE: How Age Impacts Fertility in Men and Women and How It Differs
Ethical and religious implications for women’s health
Religion within modern-day society is also debated in relation to women’s health. This is because “moral” behavior is often driven by conformity, authority, and bias. Individuals may cherry-pick Biblical passages to legitimize their own agendas and claim divine support for their views, which creates real and serious harm for others.
While religion often claims to promote morality through sanctity of life and traditional norms, it can also undermine morality. When morality is grounded in sacred texts and believed to be unquestionable, some people stop examining whether their actions actually cause others harm, weakening moral reasoning and replacing it with blatant obedience, creating stigmas, social disparities, and gendered roles throughout generations of conformity biases. These moral ideas concerning what is right and wrong offer no individualism or freedom, reinforcing inequity and control over women’s bodies and choices.
I think religion should always stay out of the legal and policy-based healthcare settings.
The need for restrictions on abortion, for example, are often framed as a moral certainty within religion, ignoring women’s autonomy, health, medical needs, and lived experiences. Personally I don’t think that complex human situations should be reduced to religious moral absolutes.
LEARN MORE: Religion and Morality
LEARN MORE: Classics of moral and political theory
The ABCs are cool!
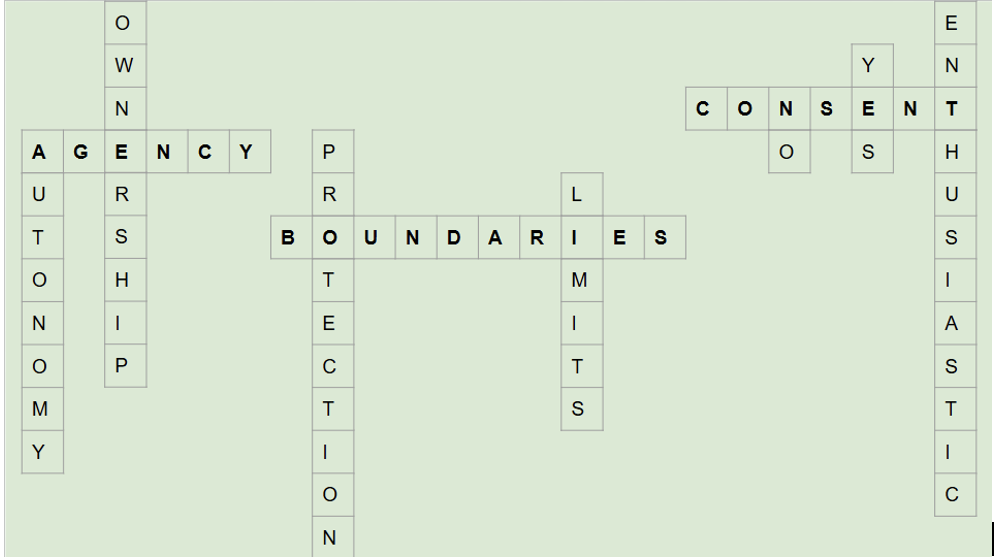
Agency, Boundaries, and Consent (ABCs) allow everyone to benefit and manage stress and self-awareness, increasing their control, empowerment, and skill at emotional regulation.
Boundaries are personal rules and limits that each person sets for themselves and others around them to define what they deem safe and comfortable in relationships, including what actions are acceptable that allow for agency over one’s own body. Teaching boundaries young, even with small things like hugs, means that people can apply the ABC’s to bigger and more serious situations in the future.
Boundaries are especially necessary for reproductive mental health and well-being. We are more than our reproductive organs. We could be successful in our careers, get multiple degrees, follow a dream, or travel, and yet people will ask, “When are you getting married? When are you having children? You don’t want your good years to pass,” as if our only success will be bearing children.
Throughout my adolescence I distinctly remember stating that I never wanted children, and being told, “But you’re so good with kids! But you have childbearing hips! You’ll change your mind. Who’s going to take care of you when you’re older? That’s selfish.” These comments impacted how I viewed myself as a woman and my sense of the meaning and value my life held within our society.
LEARN MORE (Recommended): It’s Your Body: The Young Women’s Guide to Empowered Sexual Health
Is there a difference between male and female brains?
This question was asked by a student at Fort Vancouver High School.

My main educational focus and passion is understanding the societal pressures, stigmas, mental health, reproductive disparities, and overall psychological well-being for women, so this question genuinely got me thinking deeper and further.
It is important to understand the extent to which variation exists, and how deeply experience and environment shape the brain. Men and women do not have two separate types of brains, but brains that are influenced by biology and environment. Due to proportionately larger body sizes, and the mapping of our bodies in our brains, males (on average, though with lots of individual variation) have about 10%-12% larger total brain volume.
The consensus across research finds that male and female brains differ (overall) in size and some aspects of structure, but organization matters more than size. The normal range of brain sizes, for example, does not impact intelligence, IQ, or overall ability.
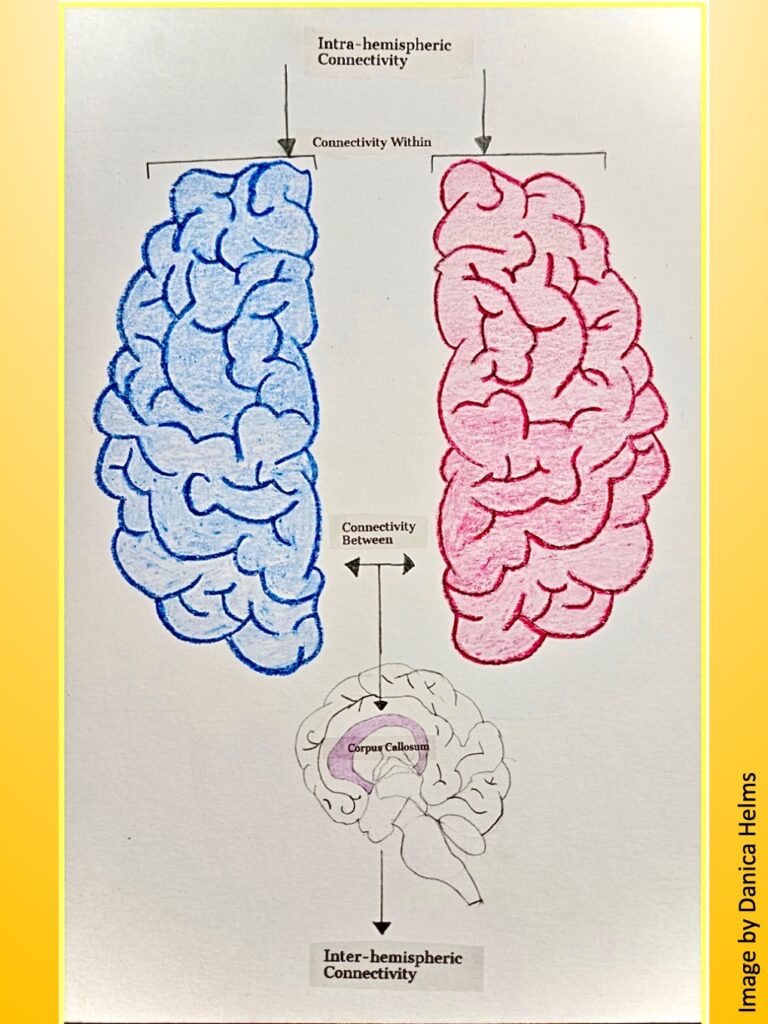
Again, on average, males tend to have larger overall brain volume and white matter. White matter is made up of myelinated axons that are responsible for communicating between brain regions. In connectome and imaging studies, males showed optimization for intra-hemispheric connections (within each hemisphere) for more focused within-region processing.
On average, women tend to have a thicker cortex and a higher proportion of gray matter. Gray matter is mostly made of neuron cell bodies and is heavily involved in processing information: thinking, decision-making, memory, and language. Across connectome and imaging studies, women show optimization for inter-hemispheric connections (between the two hemispheres), which become more integrated, coordinating information across different regions.
However, both are described in research as complementary patterns, not in terms of specific advantages or disadvantages. Men’s and women’s brains tend to be organized in slightly different ways, reflecting different strategies for processing information that are shaped by lived experiences, expectations, and so much more.
“Behavioral differences may stem from complementary roles in procreation and social structure; examples include enhanced motor and spatial skills and a greater tendency for physical aggression in males and enhanced verbally mediated memory and social cognition in females.”
LEARN MORE (Recommend): Sex differences in the structural connectome of the human brain
LEARN MORE: Two Minds: The cognitive differences between men and women
LEARN MORE: Sex Differences in Brain Anatomy
LEARN MORE: Brain Differences Between Men and Women: Evidence From Deep Learning
LEARN MORE: NIH study shows highly reproducible sex differences in aspects of human brain anatomy
LEARN MORE: Integrative structural, functional, and transcriptomic analyses of sex-biased brain organization in humans
Are women better at multi-tasking?
The idea that women are naturally better at multitasking appears mostly inconsistent with research, as many studies show that men and women generally perform similarly, rather than this being an innate gender-based trait.

Overall, humans are truthfully not well-suited for multitasking. What we call multitasking is referred to in research as rapid task switching, which tends to reduce efficiency and accuracy for everyone.
Some researchers hypothesize that women’s stronger cross-hemispheric communication could help with certain tasks that require integrating different kinds of information, such as coordinating emotional and analytical processing at once to support faster task-switching in certain contexts.

Differences that do appear are shaped more by context, expectations, experience, and life demands than by biological sex. Women are not inherently better multitaskers, but rather develop these skills because of the expectations put upon women’s shoulders. Real-world multitasking is complex, learned, and influenced by environment and responsibilities, where lab tests often measure narrow cognitive processes.
LEARN MORE: Why Women’s Brains Are Better Than Men’s At Multitasking
LEARN MORE: Women aren’t better multitaskers than men – they’re just doing more work
Women’s health requires looking beyond the question of male versus female brains, as we actually share brains that are influenced by both biology and environment.
Exploring this topic through public outreach, hormones, neurotransmitters, anatomy and importantly, our social experiences, makes clear to me that biology alone can never explain it all, and that we must continue to make changes that improve the health and well-being of women.
“I am not free while any woman is unfree, even when her shackles are very different from my own.” –Audre Lorde