

")
Post by Hailey Larson, junior undergraduate at Portland State University, pursuing a bachelor’s degree in Psychology, with a minor in Interdisciplinary Neuroscience. Hailey is currently going through the process of becoming a United States Marine Corps Officer.

This spring, I participated in outreach at both Portland and Vancouver public schools through Northwest Noggin. I loved learning what students were interested in and answering any questions they had about the brain.
On one of our first visits a student asked me how trauma affected the brain, or if there was any way to know if someone had experienced mental trauma. I was already fascinated by trauma psychology, and I felt like it would be an interesting topic to look into further.

My interest with trauma and brain trauma comes from personal knowledge of people who have gone through trauma. I also want to become a trauma therapist later down the road.
LEARN MORE: APA GUIDELINES on Trauma Competencies for Education and Training
LEARN MORE: Pursuing a Career in Clinical or Counseling Psychology
How does trauma affect your brain?
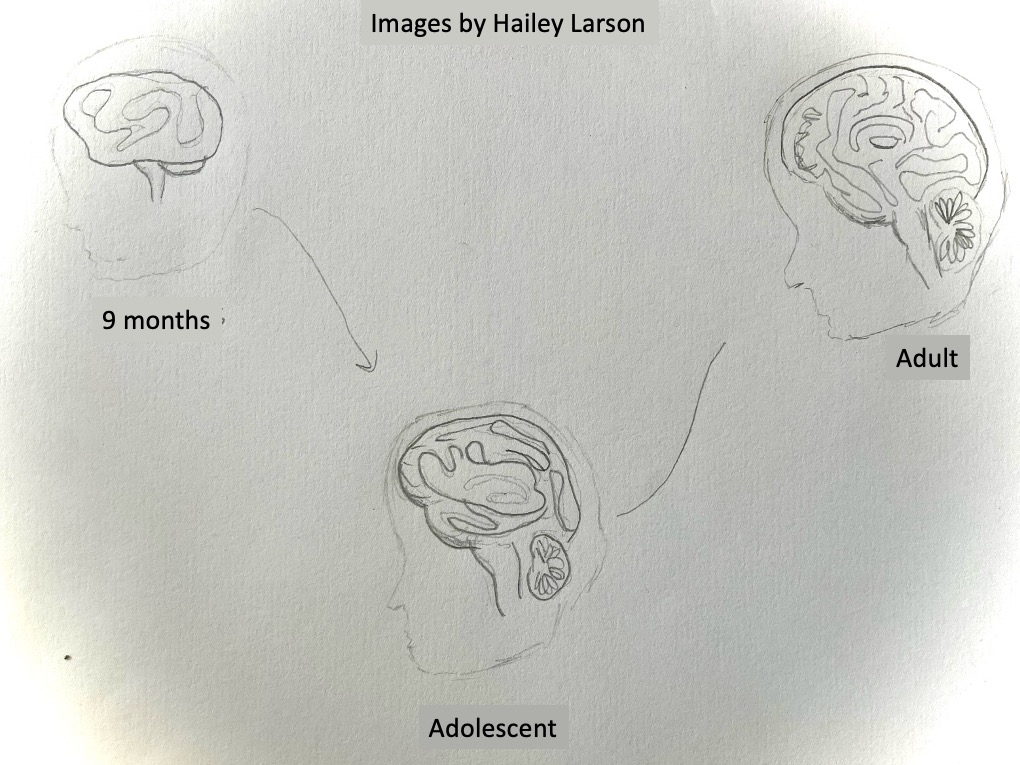
A healthy human brain undergoes a continuous process of change in both structure and function throughout one’s life. During early childhood, adolescence, adulthood, and into old age, the brain develops and matures due to genetic, environmental, and lived factors.

Because of this dynamic character, the impact of trauma, either physical or psychological, varies significantly depending on the timing of the experience. For example, early childhood trauma can disrupt critical periods of brain development, which can jeopardize the establishment of secure attachment to others, emotional regulation, and cognition. On the other hand, while traumatic experiences during adulthood may not hamper basic development milestones, they do have the capability to significantly modify neural circuits for memory, emotion, and the regulation of stress.
Traumatic events can lead to significant neurophysiological changes, particularly in regions such as the amygdala, hippocampus, and prefrontal cortex, which are locations that participate in emotion processing, memory, and decision-making.
These changes usually manifest as emotional and behavioral symptoms, including heightened anxiety, depression, aggression, or difficulties with concentration and impulse control. Cognitive operations such as attention, working memory, and executive functioning may also be impacted.
Also, trauma has a direct impact on the body’s stress response system.
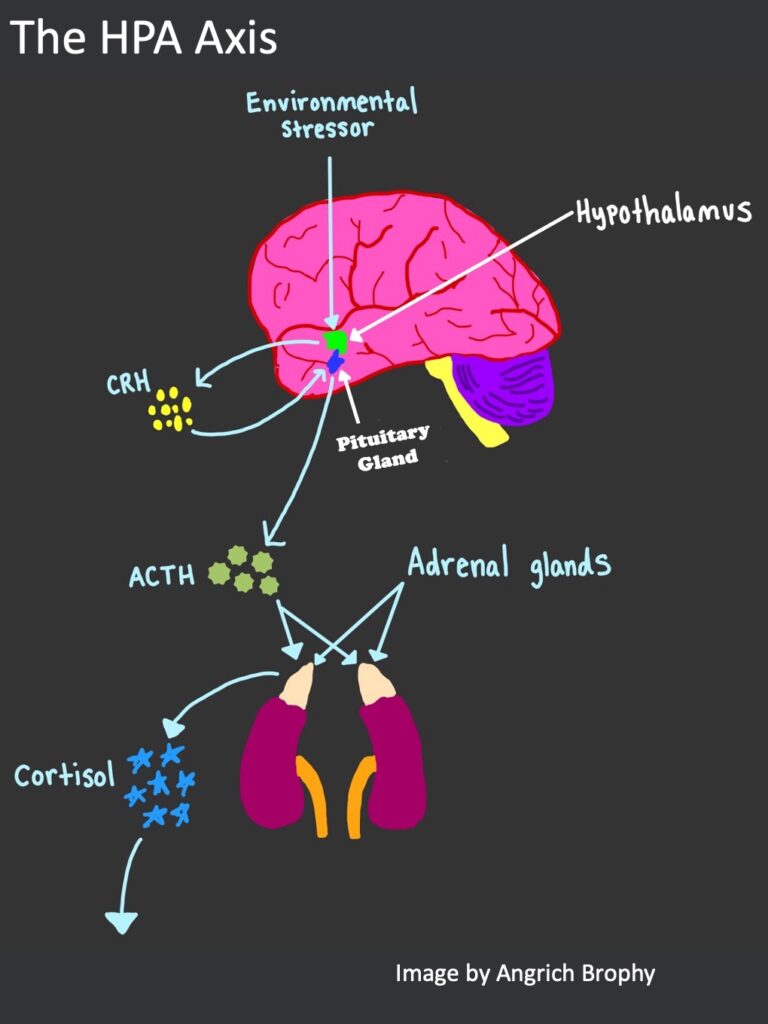
The Hypothalamic-Pituitary-Adrenal (or HPA) axis is the central stress-response system of the body, and includes the hypothalamus, pituitary gland, and adrenal glands. Under normal circumstances, the HPA axis regulates the release of stress hormones like cortisol in response to perceived threat.
The hypothalamus is located at the base of the brain, just above the brainstem, while the pituitary is located in a small bone cavity called the sella turcica (Latin for Turkish saddle), just below the hypothalamus. The adrenal glands sit on top of each kidney.
When the body senses stress, the HPA axis triggers the release of cortisol, a hormone that makes energy available, increases alertness, and turns off nonessential bodily functions.
LEARN MORE: Is stress ever good?
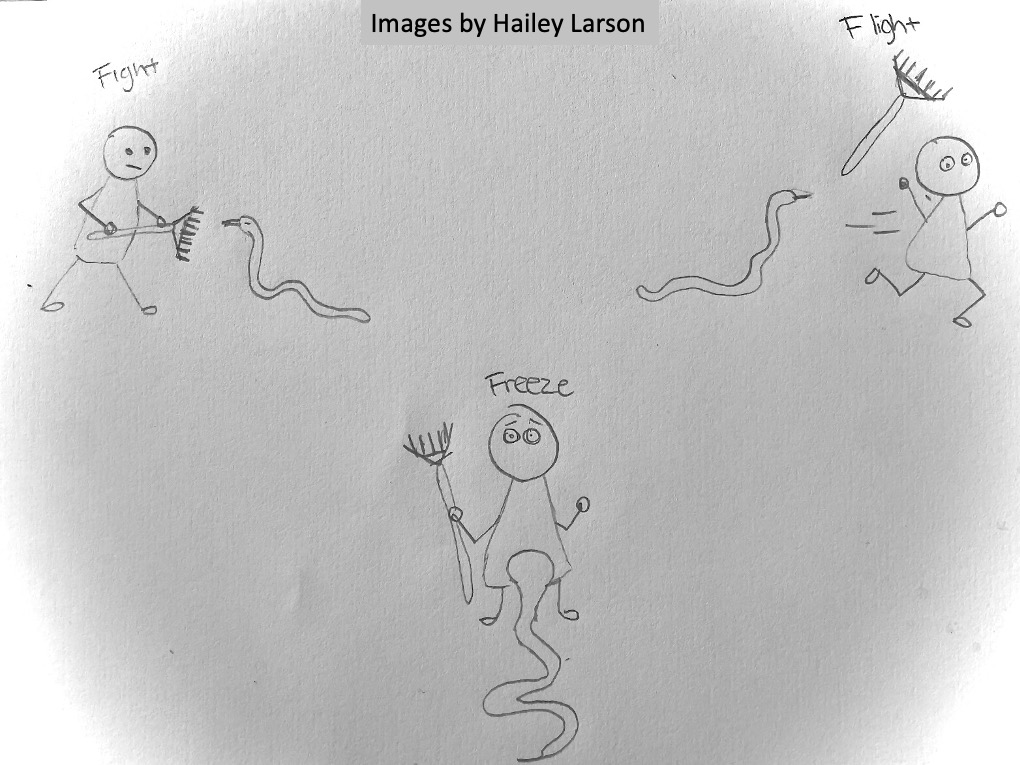
However, repeated or severe trauma can dysregulate this system, and lead to an over-aroused or “stuck” fight-or-flight response. When the brain and body are maintained in a constant state of hyperarousal, it can cause long-term physical and mental sickness, such as chronic fatigue, autoimmune disorders, and post-traumatic stress disorder (PTSD).
A high level of alertness becomes counterproductive in the long term, rendering an individual less capable of feeling secure, regulating emotions, and functioning efficiently in daily life. While stress is beneficial in the short term, prolonged stress can cause abnormally high or flattened cortisol levels. This change is linked to anxiety, depression, exhaustion, and trauma disorders including PTSD and also to underlying alterations in brain areas such as the hippocampus, amygdala, and prefrontal cortex.

LEARN MORE: The Biological Effects of Childhood Trauma
LEARN MORE: Traumatic stress: effects on the brain
LEARN MORE: Neuropsychological Consequences of Massive Trauma: Implications and Clinical Interventions
LEARN MORE: Affective Visual Circuit Dysfunction in Trauma and Stress-Related Disorders
LEARN MORE: Anxiety, fear extinction, and threat-related amygdala reactivity in children exposed to urban trauma
LEARN MORE: On the role of epigenetic modifications of HPA axis in posttraumatic stress disorder and resilience
LEARN MORE: Why Rape and Trauma Survivors Have Fragmented and Incomplete Memories
LEARN MORE: How Emotional Abuse in Childhood Changes the Brain
LEARN MORE: When Is Your Brain Fully Developed? Brain Maturity from Adolescence to Adulthood
LEARN MORE: Hypothalamus and Post-Traumatic Stress Disorder: A Review
LEARN MORE: Stress, hypothalamic-pituitary-adrenal axis, hypothalamic-pituitary-gonadal axis, and aggression
LEARN MORE: HPA Axis Alterations in Mental Disorders: Impact on Memory and its Relevance for Therapeutic Interventions
LEARN MORE: The hypothalamic-pituitary-adrenal axis in PTSD: Pathophysiology and treatment interventions
Where does trauma affect your brain?
Trauma profoundly impacts various regions of the brain, all of which are critical for our ability to regulate emotions, to remember, and to make social decisions.

Amygdala
One of the most important regions affected by chronic stress and trauma is the amygdala, which is responsible for detecting threats and generating emotional responses, including fear.
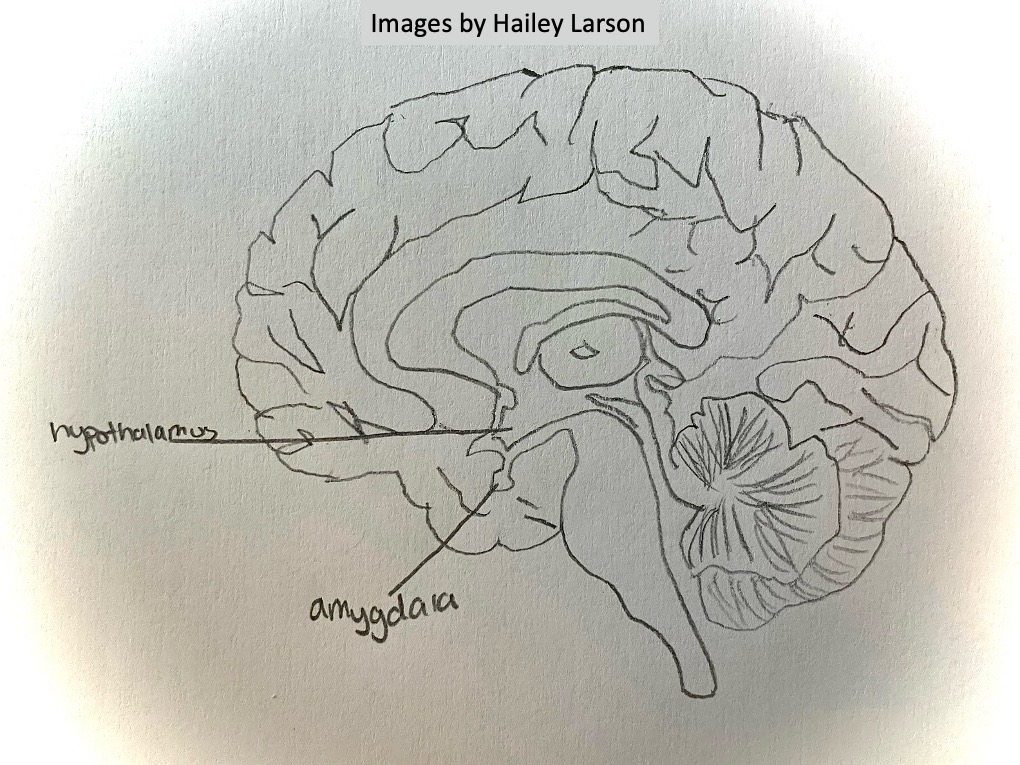
In individuals who have experienced trauma, especially chronic or severe forms such as abuse or exposure to combat, the amygdala becomes overactive. This heightened arousal can lead to increased anxiety, greater emotional reactivity, and chronic hypervigilance, where the brain is constantly on the alert for threat, although no real threat is present.
Hippocampus
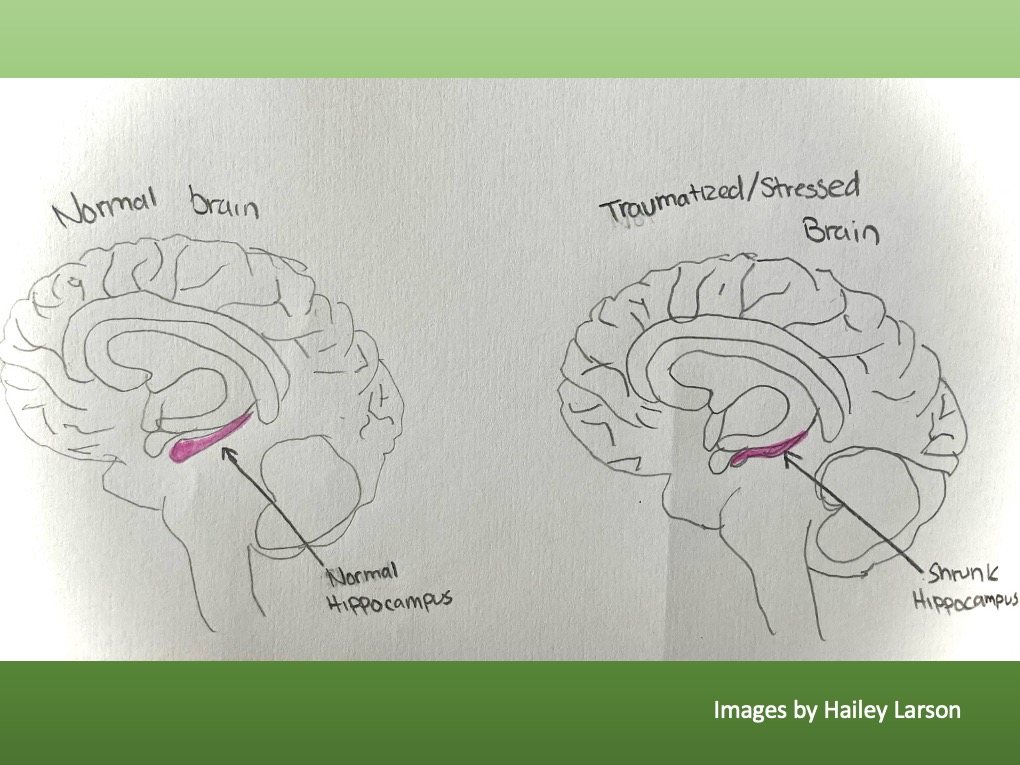
Another significant region impacted by trauma is the hippocampus, the region that forms memories of particular life experiences and helps us discriminates between past and present.
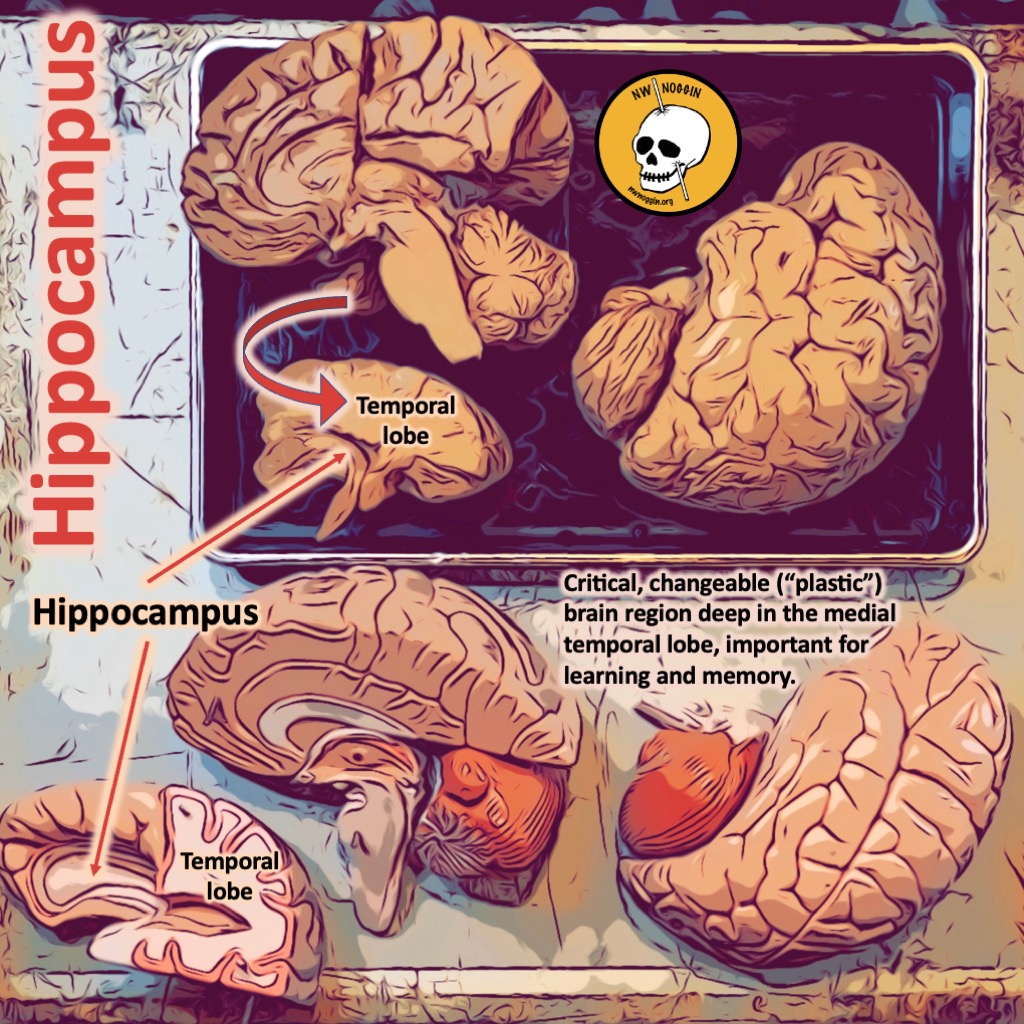
In post-traumatic stress disorder (PTSD), the hippocampus tends to shrink due to the neurotoxic effect of chronic stress and elevated cortisol levels. This loss of volume can interfere with the encoding and recalling of memories, such that it is hard to leave traumatic experiences in the past. People can re-experience past events in the here and now, resulting in flashbacks and intrusive memories.
Loss of volume in the brain here is not just a structural change, it can dramatically affect how a person thinks, remembers things, and reacts to stress. That’s why it’s a prime area of interest in studies of trauma, mental illness, and neuroplasticity.
How does trauma shrink the hippocampus? Chronic stress has the potential to do massive harm in this brain structure through a variety of interconnected biological mechanisms.
Chronic exposure to cortisol, or glucocorticoid toxicity, is one of the primary offenders.
The hippocampus contains a high density of cortisol receptors, so it is especially vulnerable to chronic elevations in this stress hormone. Over time, too much cortisol harms synaptic plasticity, weakening the brain’s ability to form and maintain connections. It also suppresses neurogenesis, the development of brand new neurons in the dentate gyrus, and causes dendritic atrophy, shrinking the “branches” of neurons and disrupting communication between them.
Stress also increases levels of glutamate, the brain’s primary excitatory neurotransmitter.
When glutamate is released in excess, it overstimulates NMDA receptors, allowing an influx of calcium into the neurons that can result in cell damage or death, a phenomenon known as excitotoxicity.
Chronic stress also decreases levels of brain-derived neurotrophic factor, a protein required for neuronal survival, growth, and plasticity. Decreased levels of this protein increase the susceptibility of hippocampal neurons to damage and lower the brain’s capacity for self-repair.
Finally, stress also activates pro-inflammatory signaling pathways, which increase cytokines which are toxic to neurons and inhibit their growth. Collectively, these effects are thought to contribute to hippocampal volume loss and to memory, emotion regulation, and stress resilience impairments.
LEARN MORE: Glucocorticoid toxicity in the hippocampus: reversal by supplementation with brain fuels
LEARN MORE: Glucocorticoids increase excitotoxic injury and inflammation in the hippocampus of adult male rats
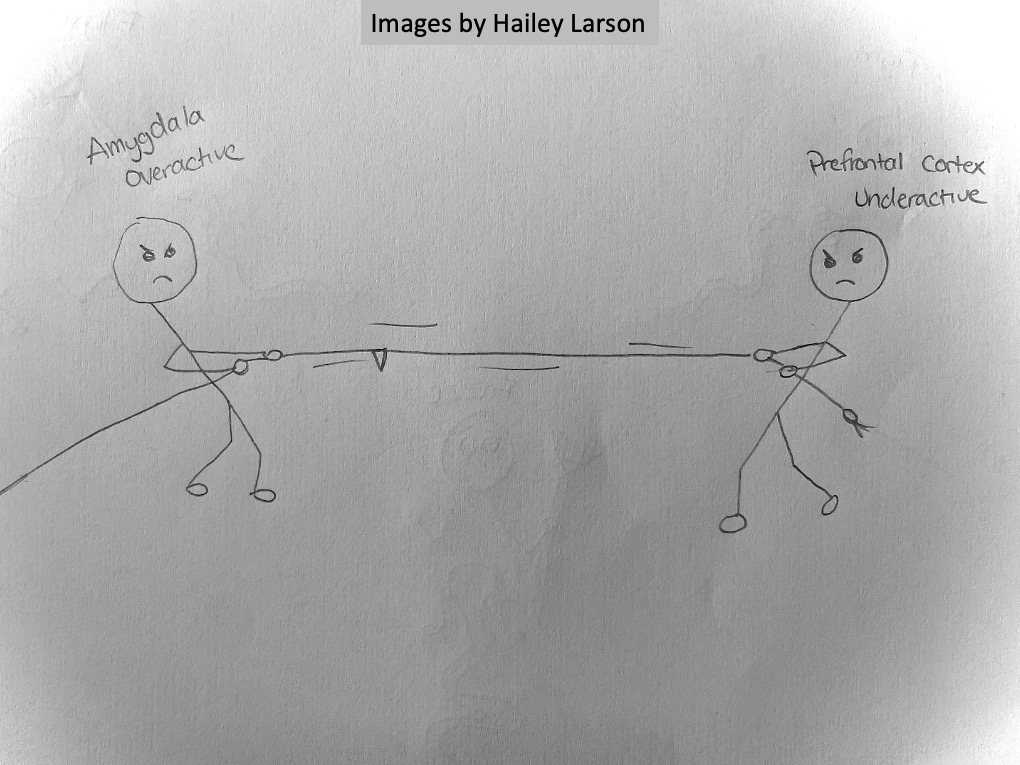
Pre-frontal Cortex
The prefrontal cortex (PFC) facilitates our impulse regulation, and emotional regulation, and is also affected by trauma. Trauma often causes this region to reduce activity, which impairs a person’s capacity for emotional control, thinking under stress or applying sound, thoughtful judgment. Subcortical areas like the amygdala can overwhelm PFC efforts to quiet the brain and consciously consider other options for a response. This is why trauma victims are not able to regulate their reactions, control their impulses, or calm themselves when they are right in the middle of an emotionally intense experience.
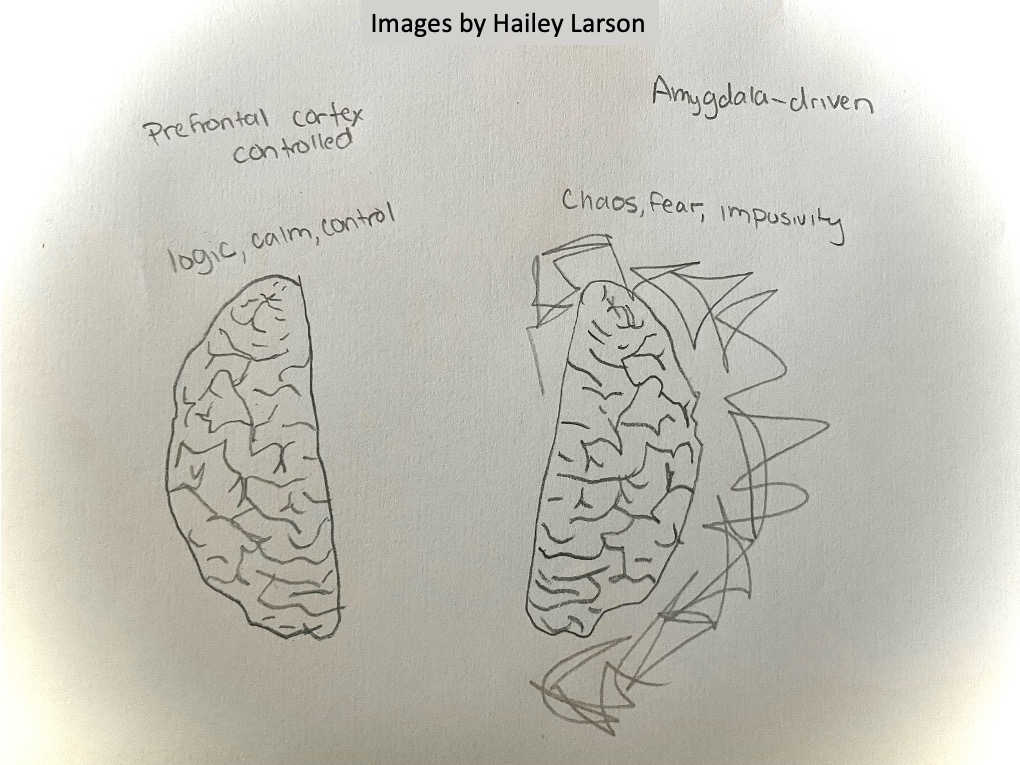
The communication between these three areas of the brain—the amygdala, hippocampus, and prefrontal cortex—establishes a critical circuit that determines how we respond to stress and perceived threats. When trauma disrupts the balance between them, it can lead to long-term challenges with emotional, cognitive, and behavioral functioning.
These brain changes account for many symptoms of trauma-related disorders, which highlights the importance of brain-based, trauma-informed care and treatment approaches to recovery.
LEARN MORE: Quantitative meta-analysis of neural activity in posttraumatic stress disorder
LEARN MORE: The association of PTSD symptom severity with amygdala nuclei volumes in traumatized youths
LEARN MORE: Blasts to the Head ‘Primed’ Brains for PTSD, Study Says
LEARN MORE: Hippocampal and amygdala volumes in adults with posttraumatic stress disorder secondary to childhood abuse or maltreatment: A systematic review
LEARN MORE: Smaller hippocampal volume as a vulnerability factor for the persistence of post-traumatic stress disorder
How can we treat this?
Several evidence-based treatments can help people heal from trauma and rewire the brain’s stress response. These therapies treat both the psychological and physiological effects of trauma, aiming to rebalance the brain and nervous system. Three of the most effective psychotherapeutic modalities are Eye Movement Desensitization and Reprocessing (EMDR), Trauma-Focused Cognitive Behavioral Therapy (TF-CBT), and Somatic Experiencing.

What is EMDR?
Eye Movement Desensitization and Reprocessing (EMDR) is a systematic, evidence-supported psychotherapy procedure intended to help people heal from trauma by recalling and then reprocessing or reconstructing traumatic memories. A significant advantage of EMDR is that it can access and modify traumatic memories that are likely to be stored in the brain in a raw, unprocessed state. These memories may be persistently vivid, emotional, and intrusive and may produce symptoms such as flashbacks, panic, or overwhelming distress when stimulated by cues that call them up.
During EMDR, the patient is asked to recall the traumatic event while simultaneously engaging in bilateral stimulation (e.g., eye movement, tapping, or alternating bilateral auditory tones) between both sides of the body. Bilateral stimulation is believed to activate both hemispheres of the brain to enable adaptive information processing. It assists in transferring memory from the limbic system, particularly the amygdala (which is concerned with emotional reactivity), to the prefrontal cortex, where better rational thought, control, and perspective can be achieved.
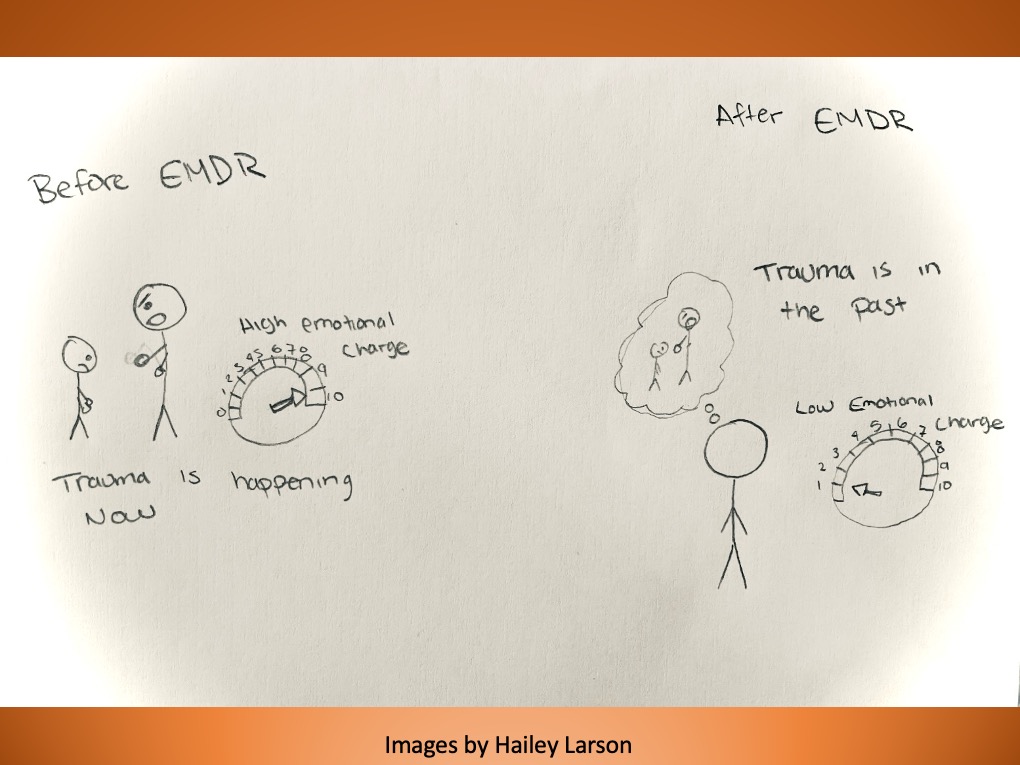
As the memory is constantly worked through in EMDR sessions, its intensity and vividness both decay. People tend to say that they feel less connected to or neutral regarding the memory. The memory is still there, but it can no longer trigger the original fear, shame, or pain. Following effective treatment, the memory is merely one aspect of the individual’s history, not something that intrudes into the here and now. This reduction of reactivity is consistent with evidence showing reduced amygdala activation and increased activity within regulatory regions like the anterior cingulate cortex after treatment.
Further, EMDR not only addresses the emotional processing of the traumatic event but also the negative self-perceptions that routinely occur as a result. For example, thoughts such as “I am helpless,” “I am unlovable,” or “I am unsafe” become embedded in a person’s self-concept following trauma. EMDR has a special phase that is focused on eliminating such maladaptive beliefs and substituting them with more positive, adaptive ones, such as “I did the best I could,” or “I am safe now.”
By helping individuals incorporate the traumatic memory into a coherent narrative, EMDR restores a sense of safety and control, so the brain knows that the trauma is not happening anymore. This shift makes healing possible, reduces the frequency of trauma symptoms like flashbacks and nightmares, and increases overall emotional resilience.
LEARN MORE: How Does EMDR Therapy Work?
LEARN MORE: How Does Eye Movement Desensitization and Reprocessing Therapy Work? A Systematic Review on Suggested Mechanisms of Action
LEARN MORE: Trauma-Focused Cognitive Behavioral Therapy: Assessing the Evidence
LEARN MORE: A FLASH OF HOPE: Eye Movement Desensitization and Reprocessing (EMDR) Therapy
LEARN MORE: Can working memory account for EMDR efficacy in PTSD?
LEARN MORE: The Predictive Processing Model of EMDR
LEARN MORE: State of the science: Eye movement desensitization and reprocessing (EMDR) therapy
LEARN MORE: How does EMDR work? A neuroscience explanation.
LEARN MORE: Understanding the Neuroscience Behind EMDR Therapy: A Path to Healing
LEARN MORE: Neurobiological correlates of EMDR therapy effect in PTSD
LEARN MORE: The working mechanisms of imagery rescripting and eye movement desensitization and reprocessing
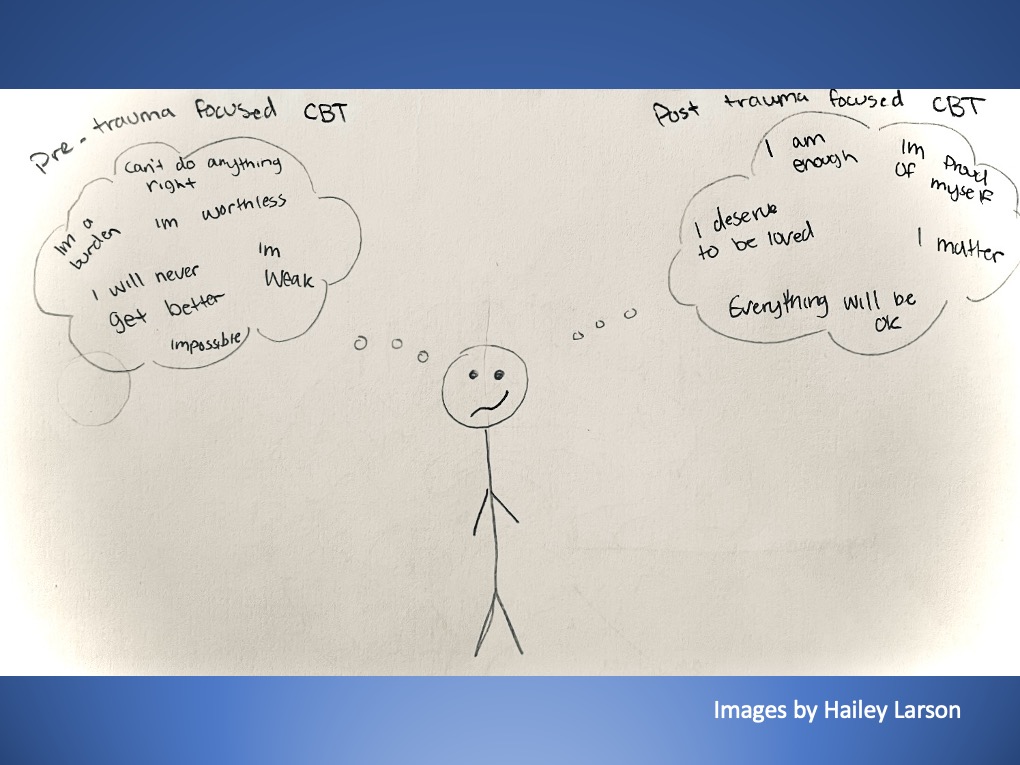
Trauma Focused Cognitive Behavioral Therapy
Trauma-focused CBT (TF-CBT) merges traditional cognitive-behavioral techniques with trauma-sensitive approaches. TF-CBT helps the individual to identify and reframe negative thoughts connected to trauma, and trains them to cope and manage emotions. TF-CBT can strengthen the prefrontal cortex in the long run, promoting rationality and emotional control, and suppressing amygdala overactivity.
LEARN MORE: Trauma-Focused Cognitive Behavioral Therapy: Assessing the Evidence
LEARN MORE: Trauma-Focused Cognitive Behavioral Therapy in 13 Urban Public Schools
LEARN MORE: Trauma-Focused Cognitive Behavioral Therapy
Somatic Experiencing
Somatic Experiencing directly addresses the physical effects of trauma by encouraging awareness of bodily sensations and exercises designed to help release stored tension in the body. It is a bottom-up process that is particularly beneficial in calming a dysregulated nervous system and allowing for the integration of traumatic experiences without being too overwhelming to the individual.
LEARN MORE: Somatic Experiencing for Posttraumatic Stress Disorder
LEARN MORE: Somatic experiencing – effectiveness and key factors of a body-oriented trauma therapy
LEARN MORE: Somatic experiencing: using interoception and proprioception as core elements of trauma therapy
Stories matter
My interest in brain trauma began with an easy question: Why are people so uniquely gorgeous in how they respond to hardship or stress?

My curiosity grew through my experience with Search and Rescue and my desire to be a part of the United States Marines, both experiences which placed me into situations that allowed me to face reality concerning trauma. But what actually nailed my life goal was my desire to be a trauma therapist. I wish to help people heal not only emotionally but neurologically. Trauma lives in the brain as much as the heart.
By doing this outreach work, whether I was showing people how helmets protect the brain or guiding students through the workings of the prefrontal cortex, I discovered how eager people are to learn what’s actually going on in their own heads.

But what engaged me more with this subject wasn’t the science itself – it was the stories.
Students’ testimonies of having survived violence, adolescents wrestling with anxiety, and (outside these outreach experiences) some adults I’ve met who carry intangible wounds. A few students shared their own personal histories with me, including recollections from their childhood that duplicated the very symptoms and patterns I was researching at PSU. These experiences reminded me that we all require language with which to speak about our misery, and I believe that science offers that language. What I’ve come to understand is that trauma is not just a psychological issue; it’s a biological one. It changes how the brain is wired, altering memory, emotional regulation, and behavior.
The brain, however, is not fixed. It is capable of adaptation and healing. This project, for me, has gone beyond education. It has become a form of compassion through understanding. I want to help people see their brains not as lacking, but as adaptable, strong, and in need of nurturing. Trauma-informed brain outreach is now a calling.
